― 文献名 ―
Are journal clubs effective in supporting evidence-based decision making? A systematic review. BEME Guide No. 16.
J. Harris et al. Med Teach 2011;33(1):9-23
― この文献を選んだ背景 ―
Since 2012, weekly lecture for residents have launched and I’ve performed interactive lecture and on-site practice of about EBM for three times. In the evaluation with questionnaire, I found that residents felt somewhat difficult to perform 5 step of EBM in their daily practice. Therefore, I would try to improve the educational method and strategy this year. For the first step, I search for the best evidence of teaching EBM, and found this paper.
― 要約 ―
Research background;A journal club (JC) is an interactive approach to making sense of evidence, which is commonly defined as ‘a group of individuals who meet regularly to discuss the clinical applicability of articles in current medical journals’ (Linzer 1987).
Their popularity can be attributed to a number of perceived benefits -they help students and practitioners to keep up to date with health care literature, become more critical consumers of research evidence, and become better practitioners. Positive attitudes about JCs have changed little over the past 15 years.
Although education research would support a JC approach, there is little direct evidence that JCs are actually effective in reaching their stated goals.
Research Question;Is the JC effective in supporting EB decision making? Is it possible to determine which elements of a JC contribute to effectiveness?
Search strategies;The search strategy was developed using Medline (Table 3) and adapted for the requirements of other databases. Bibliographies of relevant publications and review articles were scanned and relevant references were retrieved. No language restrictions were applied.
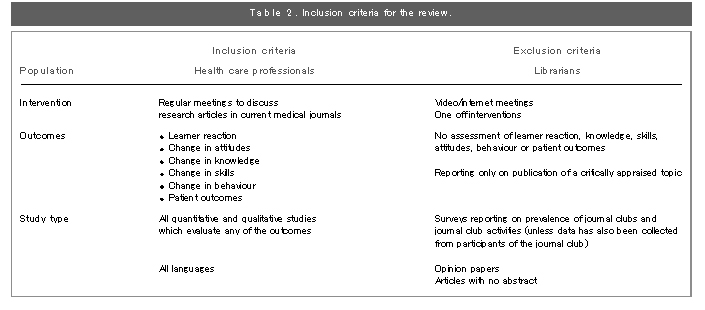
Inclusion/exclusion criteria:See Table2.
Findings:18 papers were included in the final review. Of those, 17 were for postgraduates and 1 was for both undergraduates and postgraduates. Since there was a wide range of heterogeneity of the JC intervention, authors judged it was difficult to perform meta-analysis.
(1)Main findings;The included studies reported improvements in reading behaviour (N= 5/11), increased confidence in critical appraisal (N=7/7), improved test scores on critical appraisal (N=5/7), and increased ability to use findings in clinical practice (N=5/7). They concluded that they couldn’t judge JCs are effective in supporting EB decision making, because only seven studies attempted to measure this endpoint and they relied on self-report.
(2)Methodological weaknesses are below. 1.The description of the interventions lacks attention to detail, preventing adequate replication. 2.There was a paucity of learner assessment and few validated tools were used for quantitative assessment. 3.The large variation in JC design and delivery limits comparison.
(3)Identifying active ingredients; Analysis of the various elements contained in JCs produced a cluster of elements that may contribute to the overall effect. These were termed active ingredients, and included mentoring, didactic support, use of structured review instruments, adhering to principles of adult learning, using multifaceted approaches to learning, and integrating learning with other academic and clinical activities.
(4)Implications for practice
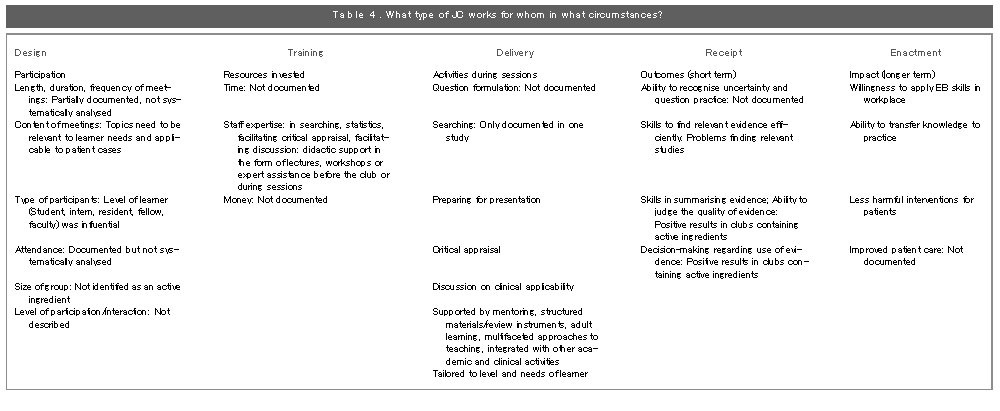
Our review illustrates that JCs are used widely across different sectors of the healthcare and used in a variety of different ways. Active ingredients are found at each stage of the educational intervention (The author applied five elements model of educational intervention and describes the results of this review about each facet in Table 4).
For example, if a JC is being designed for residents, the content should be directly applicable to patient cases they find problematic, enabling application of evidence in a real-time setting; didactic support could be provided based on an educational needs assessment (e.g. for statistical support). Critical appraisal and discussion of clinical applicability could be facilitated by senior clinicians who are in supervisory positions, enabling the transfer of discussion into practice.
― 考察とディスカッション ―
Now I plan on-line EBM WS for residents this year, this article has given me several hints. Although some of those are same as other educational sessions like adult learning and multifaceted approaches to teaching, others have some practical implication for me.
1. I would like to pay more attention on individual learners’ needs. I’ve already sent some questionnaire to know their knowledge and practice of EBM.
2. I would like to change the contents more relevant to their daily patient cases. I will discard the discussion based on the case scenario and start with gathering and evaluating their daily clinical questions from the first session.
3. Mentoring is important. I would try the hands on session of EBM STEP1 to 3. (This part was on-site activity last year.)
4. I would like to introduce more structured material for critical appraisal.
5.The support of ‘on-site’ educators is imperative. I ask for your support.
Do you manage journal clubs in your clinic? If you have, how do you manage it? Is there some implication for you?
↓ 画像をクリックすると全体が表示されます。
開催日:平成25年7月10日