【文献】
著者名:Alison Dobbie,MD.et al.
文献タイトル:Evaluating Family Medicine Residency COPC programs Meeting the challenge.
雑誌名・書籍名:Fam Med 2006
発行年:38(6):399-407.
【要約】
<Background and Objectives>
We conducted a review of the evaluation literature and outcomes from community-oriented primary care (COPC) programs in US family medicine residencies since 1969.
<Methods>
We used a Medline and ERIC search for “community-oriented primary care” in English from 1969-2005.
<Results>
Twenty-two articles were found that concerned US family medicine residency COPC. Selection process describes in table1.Finnaly, Eight descriptive and eight evaluative papers described 14 residency COPC programs. Teaching and learning methods included block and longitudinal rotations and COPC projects. Evaluation methodologies included one quasi-experimental control group study, pretests and posttests of knowledge and attitudes, focus groups, and semi-structured interviews. Reported outcomes included changes in residents’ knowledge, attitudes, and behaviors; effect on graduates’ career choice and future practice; and impact on patient care and community health.
<Conclusions>
Few studies have evaluated residency COPC programs. Evaluation has been less than rigorous, with variable results, but at least one study indicates positive outcomes at each evaluation level. More residency programs must evaluate and disseminate outcomes from their COPC projects to determine the value of COPC to residents, colleagues, community partners, and funding agencies.
<Recommendations–Designing a COPC Evaluation Plan>
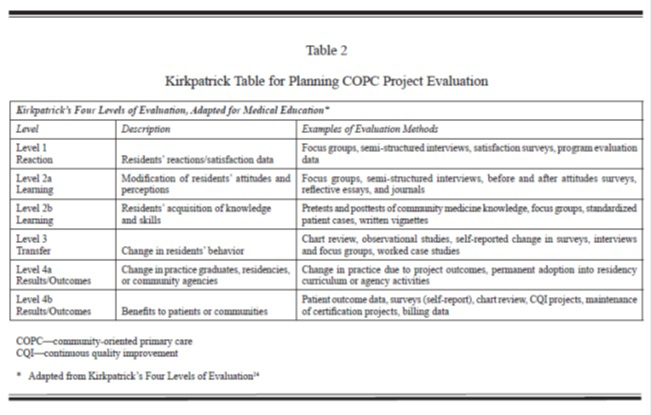
We recommend that faculty design their evaluation plan before implementing any residency COPC project, because data are more difficult to gather after the event, and the opportunity to gather baseline data is lost. We recommend that faculty design a plan addressing all four of Kirkpatrick’s levels of evaluation, as demonstrated in Table 2.
Level 1 data (reaction) measure course process outcomes, such as whether residents enjoy the learning experience, believe the content and teaching methods to be appropriate and well taught, report the program to be well organized and efficient, and consider it a useful contribution to their training.
Level 2 data (learning) describe changes in residents’ COPC knowledge and attitudes. In 1999, Oandesan validated a 20-item survey that can serve as a pretest and posttest of residents’ attitudes to COPC. Donsky published a COPC questionnaire in 1998 that can be used as a pretest and posttest of knowledge and attitudes, although this instrument has not yet been validated. Qualitative methods for evaluating learning include focus groups, semi-structured interviews, written case exercises, and reflective essays and journals.
Level 3 data (transfer) concern changes in residents’ behavior and/or clinical practice. Behavior change can be measured through direct observational studies, chart reviews, electronic health record searches, and/or selfreports in written or electronic surveys. Self-reported changes in behavior represent much weaker types of Level 3 data than objective measures such as direct observation or chart review.
Examples of Level 4 data (results and outcomes) include changes in graduates’ clinical practice resulting from the COPC projects, permanent adoption of the COPC program into the residency curriculum, and measurable effects on community agencies or practice populations. The effect of the COPC program on graduates’ practice behavior can be measured by telephone, electronic, or mailed surveys 1 to 2 years
after residency. Effects on community agencies can be measured by semi-structured interviews or focused group.
【開催日】
2012年4月26日