【文献名】
著者名:島崎謙治
文献タイトル:日本の医療 制度と政策
発行年:2011, 東京大学出版会
【要約】
序章 問題の所在と分析視角
(1)レーショニング問題
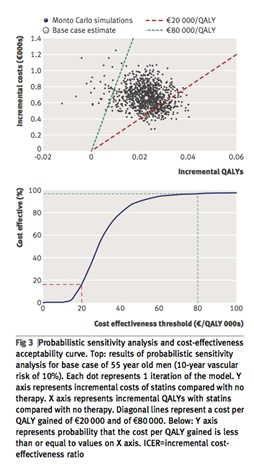
米国の「オレゴン・プラン」(※費用対効果を数値化し予算制約上一定のライン以上でなければ給付対象外とする州法)は医療のレーショニング(優先順位付け)問題に踏み込み波紋を呼んだ。多数者の尺度で少数者を排除するのは社会正義上問題がある一方、医療資源が無尽蔵でないという制限もある。日本においても医療技術の革新や高齢化の進展に伴い医療費の増加は不可避であるが、かつてのような経済成長は見込めない。
(2)日本の人口構造の変容と医療政策
老年従属人口は2005年30.5%(3.3人で1人を支える)、2030年 54.4%(1.8人で1人を支える)と急激に増加する。団塊の世代が2024年に後期高齢者となるからである。これに伴い多死社会が到来し2005年 108万人から2030年 160万人が死亡する。未婚の1人暮らし高齢者は2005年80万人から2030年 290万人となる。医療費は医療の進歩に伴い自然増があり、年率3%とすると2030年の国民医療費は78兆円(※2009年の国民医療費は36兆)。少子高齢化により経済成長立は引き下がり、年平均経済成長率が1%、医療費伸び率3%とすると、国民医療費のGDP比は2030年 12%程度となる(※2009年 10.6%)。
以上より、高齢化の進展や医療技術の革新に伴い医療費の増加は不可避である一方、高い経済成長は期待できない条件の中で、世代間公平に配慮しつつ財源確保を図り、労働力が減少する中で質・量ともに安定的に医療を供給しなければならない。
(3)医療政策の目標と選択
①医療の質、②アクセスの公平性、③コストが評価基準である。何を守り、何を攻めるか。日本の特徴としてa. 職域保険と地域保健の2階建てで国民皆保険を実現、b. ファイナンスは「公」、デリバリーは「私」中心、c. フリーアクセスの尊重、が揚げられる。これにはここに至る歴史がある。
歴史:
医制
1874年制定。西洋医学に基づく医学教育と医師開業免許制を樹立した(※それまで漢方医は免許にあたるものが必ずしも存在しなかった)。自由開業医制度はここで敷かれたことになる。
健康保険法と国民健康保険法
1914年の第1次世界大戦時に工場は飛躍的に発展し労働者数は急増した。こうした背景のもと、健康保険法は労働情勢が緊迫の度を強める中で労使協調・産業平和を目的とする労働政策立法としての性格を色濃く有していた。本来社会保険がなじみにくい農民などを対象とする旧国民健康保険法が1938年に制定されたのも、健保法が先立って制定されていたことが1つの要因になっている。日本医師会は健保法実施に当たり団体自由選択主義の採用を強く要望しており、行政当局としては制度を円滑に実施するために医師会の協力が必要であり、その意向を尊重したと考えられる。これはフリーアクセスの基礎がここで築かれたという意味で非常に重要である。旧国保法は組合を保険者とした強制力のない保険方式であったため機能しなかったが、1961年に市町村は原則として国保事業を実施することとなり国民皆保険が確立された。戦後となりようやく防貧施策を講じる準備が出来たこと、1956年当時の推計によると総人口の31.9%が保険未適用状態におかれており、これらのことから政治プロセスに国民皆保険が上った。
※強制加入制度は社会保険という性格上なじまない部分もあるが、逆選択の抑止という面では情報の非対称性の大きい医療ファイナンス面では優れている。反面、医療デリバリーは「私」中心、出来高払い、フリーアクセスのため逆選択が生じ得る状況と言える。
老人福祉法
国民皆保険達成後の1963年に制定されたため、医療から大幅に遅れて福祉が拡充してきた。福祉政策の立ち後れ、老人医療費無料化、医療機能分化の不徹底などが社会的入院と長い在院日数の原因と考えられる。
展望:
医療機関の機能分化と連携
欧米諸国に比べ日本の医療機関の機能分化は十分に進んでいない。医療機能の未分化(※ケアミックスなど、歴史としては戦後医療の量的拡大に重点がおかれたこと)、医療と介護・福祉の混合(※社会的入院など、歴史としては上述「老人福祉法」参照)、病院の外来部門と診療所の競合(※歴史としては日本の病院は診療所が大きくなったものが大半で法制的にも病院は診療所の一部と位置づけられていた)などがある。これらの結果、日本の病院は①数が多い、②平均在院日数が長い、③病床当たりの医師及び看護スタッフが少ない、などが生じている。労働節約的な病院環境は医療安全の面でも勤務者の「立ち去り型サボタージュ」の面でも妥当ではない。病院機能の分化・集約化を進め、一方で居住系サービスの整備が必要である。高齢化社会において複数の問題に対応し、居住系サービスへの医療にも対応し、よく訓練された結果ゲートキーピング機能を発揮することを期待できる、家庭医が必要となる。
※家庭医医療過疎地域で活躍し地域住民から高い評価を受けている実例として、島崎(2007)『医療等の供給体制の総合化・効率化に関する研究』(厚生労働科学研究補助金/政策科学推進事業 平成16-18年度総合研究方向書)より島崎(2007)「北海道更別村におけるプライマリ・ケアの実践とその効果評価」、及び中川貴史(2007)「公的有床診療所を運営維持していく必要性とその問題点-寿都町立寿都診療所の事例」が引用されている。
【開催日】
2012年8月29日