【概要】POLSTとは
・Physician Orders for Life-Sustaining Treatmentの略語
・’End of life'(敢えて終末期と訳しませんでした。)における医療の質の改善のために考慮されたプログラムで、患者の希望を聞き出すための効果的なコミュニケーション、色彩がはっきりした紙への行いたい医療の記載、その希望に対する医療者の遵守が土台となっている。
・1991年に、オレゴンにて延命治療に対する患者の希望が尊重されていないことに問題意識を感じた医療倫理分野の専門家が活動を開始し、1995年にForm(書式)が初めて出版された。
・現在では、オレゴン州では、POLSTを用いていることが、ケアの基準として受け入れられており、全てのホスピスと95%の高齢者施設において採用されている。2004年にはPOLSTのメンバーが、USの国のタスクフォースとして、国内への流布・政策整備・リサーチの実施のために、活動を開始した。
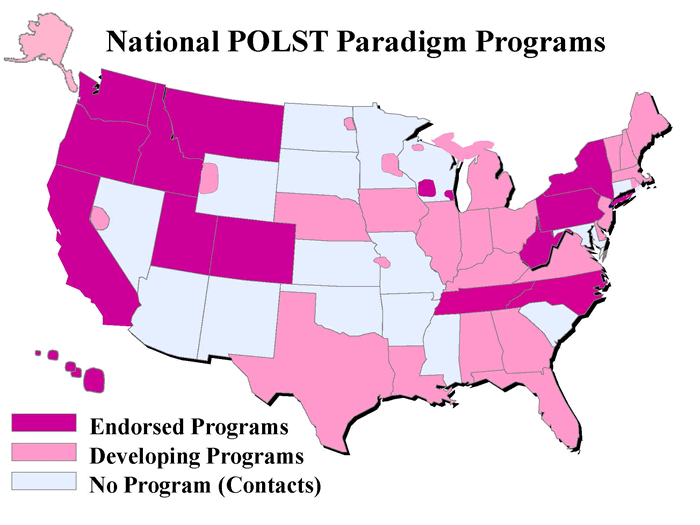
・現在のUSAにおける、POLSTプログラムの採用状況は図1のとおりである。
【POLST Formの記載内容】
・「POLST Oregon sample」「POLST newest 日本語」にそれぞれオレゴン州のサンプルとその日本語訳があります。
・確認するのは主に以下の3点
①心肺停止状態の時のCPRをするかどうか 日本での従来的なDNARかどうか、に該当します
②①ではなかった時の、医療をどこまで希望するか
1.緩和処置のみ施行 ;対症療法のみ
2.限定された医学的処置の施行;通常の治療を行うが、気管内挿管・長期の生命維持・ICU治療などは行わない
3.積極的な治療 ;侵襲的な処置も全て行う
③人工的な栄養と輸液の投与
1.一切行わない 2.期間を限定して行う 3.長期的に行う
④抗生物質投与(州によって項目として独立していない場合もあり)
1.使用しない。症状緩和のための場合は行う
2.侵襲的な投与は行わない(筋肉内・静脈内は行わない) 3.積極的に行う
⑤話し合いに参加したメンバーの記載
【実際にどのように使用されているか?】
・オレゴン州では、ある年齢を超えた患者全員に対して推奨されているとのこと。電子カルテのAlertとも連動しているクリニックもあるようで、聴取していない場合は、Alertが出るようにされているところもあるとのこと。
※HPでみる限りは、オレゴンは非常に進んでいるようで、プログラム全体としてPOLSTの推奨としているのは、「進行した慢性進行性の疾患を持っている人、翌年に死亡あるいは意思決定能力が失われる可能性がある状況にある人、また、自分が受けるケアについて意思表示を明確にしたいという要望を持っている高齢者ならだれでも」、となっています。
参考;http://www.ohsu.edu/polst/developing/core-requirements.htm
・実際には、希望を書いた紙を、平時は患者自宅の冷蔵庫などに貼ってあって、救急隊が現場到着した際に、その紙を同時に持っていく、というような感じになっているそうです。(外出時はどうしているのかは聞いてきませんでした)
・法的効果も認められており、実際にPOLSTに反して蘇生をして、生き返った当人が訴訟をしたケースもあるとのこと。
・記載はもちろん強制ではなく、患者(あるいは代理人)の自発的な判断に基づく、とあります。
・延命治療への配慮は全ての患者においてなされるべきだと日ごろから感じている。内科的疾患で入院した際にDNARを確認した際に、「今まで話し合ったことがない」と答えた家族には退院後に一度きちんと話すように勧めたり、悪性疾患の診断を受けている患者の定期外来で、近い話題が出たら、確認してカルテに記載するよう努力はしていた。
・このようなフォームの活用することで、家族・本人との話し合いの場は持ちやすくなるし、より具体的な話をする機会を持てるだろう。継続性や関係性構築に長けている家庭医なら、「不要な心配」をかけることなく話題を切り出す役割としては適任と思われる。
・しかし、このようなフォームが本当に効力を発揮するためには、多彩な段階の治療への要望に対応するための複数の場(ホスピス・入院病床)や、それに寄り添える価値観を持ち、多彩な段階の治療を実践できる医療スタッフが存在することが必要だろう。POLSTのようなシステムと実際の受け皿が両輪になって、初めて走り出すもので、片方だけの過剰な整備では、フォームを形骸化させるもととなる。
・その一方で、こうした類のイノベーションにおいては、フォームの導入が、もう一方の「車輪」の整備のきっかけになる可能性(例えばACLSのように)があることも鑑みる価値はあると思う。現場で患者の個別化されたケアの実践に取り組み家庭医としては、システマティックでなくとも、出来ることがあるように感じる。
例えば、我々にでも以下のような活動は出来るかもしれない。
都市部;自分が受ける治療に対して希望があり意識が高い患者とのコミュニケーションに利用する
郡部;こうした概念自体の存在をチームでシェアして、特にリスクが高くかつ地域から出ていく可能性が低い集団(グループホームや特養の利用者)に関わる職種と勉強会やシステムの導入を試みる
・皆さんの普段のこうした分野でのプラクティスや工夫・実践・経験についてお伺いしたい。
【開催日】
2011年12月7日