― 文献名 ―
Ketan Dhatariya. Uncertainties: Should inpatient hyperglycaemia be treated? BMJ 2013;346:f134 doi: 10.1136/bmj.f134
― この文献を選んだ背景 ―
Usually, we try to control blood glucose of patients who are admitted with acute illness.
But after reading this article, I found that this is not confirmed with good evidence and realized the importance of knowing that some of our usual care may lack sufficient evidence.
― 要約 ―
Two large scale randomised controlled trials in the 1990s were the first such trials to show that the control of blood glucose helped to prevent long term complications in people with types 1 and 2 diabetes.1 2 Glucose concentrations can rise not only in people with pre-existing diabetes, but also, for short periods, in people without the condition–in particular, during times of acute illness, when it is called stress hyperglycaemia.3
Data show that raised blood glucose concentrations in people with and without a previous diagnosis of diabetes are associated with short term harm. However, whereas the benefits of good glycaemic control over a long period in people with diabetes are well established, uncertainty remains about whether treating transient hyperglycaemia, in particular in hospital inpatients, makes any difference to short term outcomes.
What is the evidence of the uncertainty?
Since the two trials in the 1990s,1 2 other studies have also shown that hyperglycaemia in inpatients with and without pre-existing diabetes is associated with poor outcomes. However, most trials were observational, with only a few randomised controlled trials. A meta-analysis of 34 randomised control trials assessing perioperative insulin infusion in 2192 surgical patients concluded that “perioperative insulin infusion may reduce mortality but increases hypoglycaemia in patients who are undergoing surgery.”5 However, only 14 of these studies included patients with diabetes, with 13 studies
excluding them and the rest not reporting whether patients with diabetes were included.
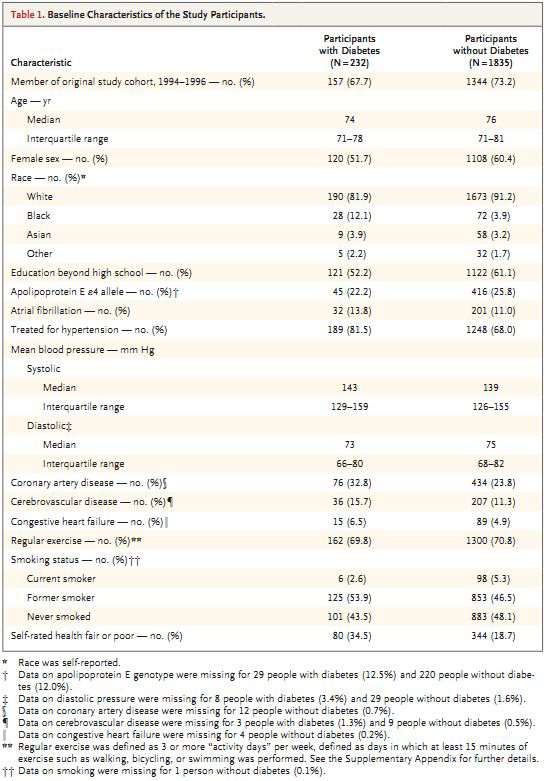
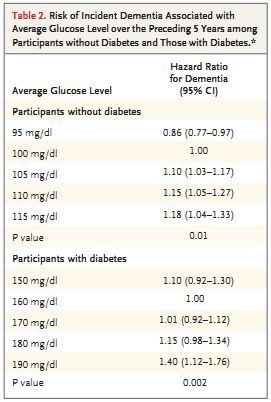
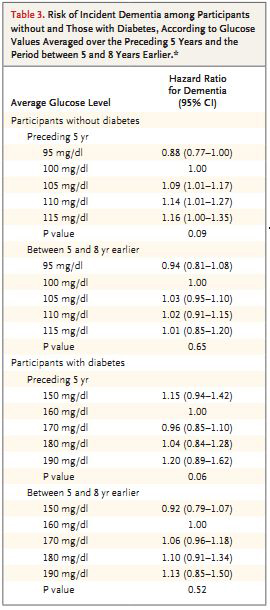
Observational data from an unselected cohort of over 1500 acute general medical admissions with and without diabetes showed that length of stay, readmission rates, and 30 day mortality rates rose with higher blood glucose concentrations.6 Other observational evidence from hospital episode statistics based on discharge coding of over four million patients showed that those who also had diabetes stayed in hospital the longest, regardless of the specialty.7
People with stress hyperglycaemia may be at risk of developing type 2 diabetes in the long term. However, evidence from intervention studies is sparse or conflicting on whether aggressive treatment of the hyperglycaemia during a patient’s hospital stay makes a difference to short or long term outcomes or even affects outcomes related to their cause for admission. Indeed, data from well conducted large randomised controlled trials and observational studies show that the use of glucose lowering agents–in particular, insulin–are associated with increased levels of harm, in the form of severe hypoglycaemia.10 11
A few randomised controlled trials show that short term, tight glycaemic control using insulin therapy in intensive care seemed to reduce mortality, infection rate, and length of hospital stay.12 13 Other well conducted randomised controlled trials in intensive care patients have been either equivocal14 15 or associated with harm, with the largest such study of over 6000 patients showing that tight glycaemic control was associated with higher incidence of severe hypoglycaemia and increased mortality.16
There are good theoretical reasons why glucose reduction with insulin should be beneficial, with reductions in endothelial dysfunction, immune dysfunction, and the maintenance of adequate vasodilatation.20 But insulin use in any patient with hyperglycaemia is fraught with problems and is often used incorrectly or ineffectively–the use of subcutaneous “sliding scales” being one such problem.21 Precipitating severe hypoglycaemia by aggressive glucose lowering with insulin is a major concern.
Uncertainty also remains about the glucose targets that should be aimed for and the best agents to achieve these.
The data presented show that high glucose concentration in people with and without diabetes is associated with poor outcomes. However, as the author found no directly relevant systematic reviews it remains to be determined if the raised blood glucose is the cause of the poor outcomes or if it is just an epiphenomenon.
What should we do in the light of the uncertainty?
If the patients are found to be hyperglycaemic then efforts should be made to control their glucose concentrations on the basis of pragmatic consensus documents drawing largely on the best available observational data previously described.
開催日:平成25年10月16日