―文献名―
Norbert Donner-Banzoff, et.al.The Phenomenology of the Diagnostic Process: A Primary Care-Based Survey. Medical decision making. 2017; Vol1:27-34
―要約―
Introduction:
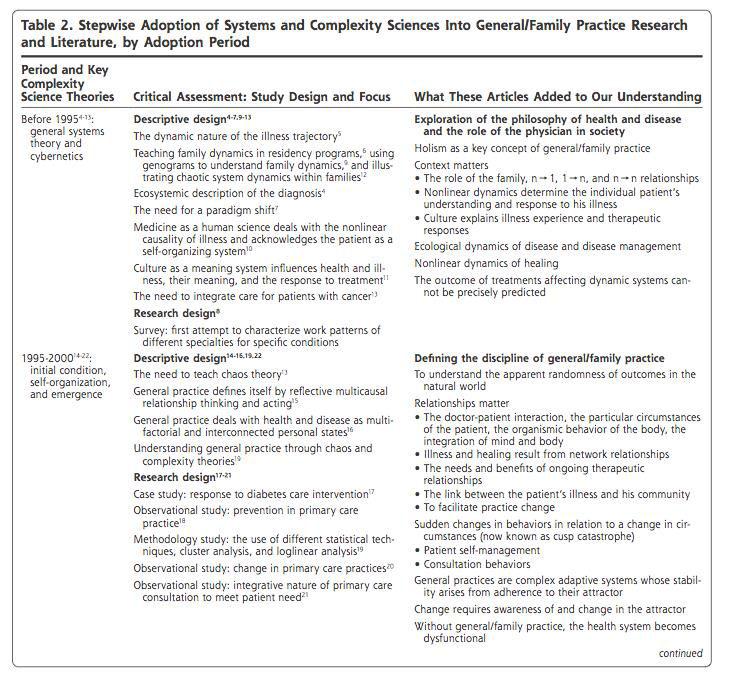
診断を行う臨床家にとって患者の言葉や病歴、疾患の有病率、視覚的な印象、身体診察の所見など莫大な情報が得られる。人間の脳は限界があり、多くの情報はノイズとなっている。ではいかに情報を収集し、選択し、重みづけし、無視しているだろう?いつ情報収集をとめ、続けているだろう?医学界で最も影響力のある臨床推論のモデルはElsteinらの提唱した仮説演繹法となっている。このモデルでは早期に診断仮説が形成されるが、診断仮説が生まれる前に起こるプロセスはわかっていない。一つかそれ以上の仮説が受け入れられるとき、臨床家は数百から千から3つか4つの説明可能な範囲へ狭めている。私たちはデータ収集の最初の段階で中心的な役割を‘Inductive Foraging’として提唱している。
私たちの目的は総合診療医(以下、GP)が診断に用いる認知戦略を明らかにすることだった。結果に基づき、数多くの鑑別を考慮しないといけないGPやそれ以外のセッティングでの現象学を提示する。

Method:
ドイツのヘッセン州マールブルグ-ビーデンコプフ群で勤務し、5年以上の臨床経験と卒前、卒後の教育経験を有する12人の常勤のGPへ研究への参加を依頼し、全員から同意を得た。それぞれのGPの3.5日の勤務を評価した。患者は症状や可能性のある診断とは無関係に組み入れられた。慢性疾患の定期通院や今回の受診前に診断された疾患の再診といった、診断とは異なる理由での受診は除外した。
参加したGPはそれぞれの患者へ研究について説明し、研究への参加と診療のビデオ録画への文書での同意を得た。同意後にGPは通常の診療を行い、その後に診断推論を説明してもらうため半構造化面接を行った。インタビューも診察と同様にビデオ録画を行った。
診療とGPへのインタビューは言葉通りに文字起こしされ、質的データ分析ソフトのMAXQDAによってコードされた。過去に出版された研究を引用し、GPの診断推論と情報収集の振る舞いを描出するカテゴリ化を行った。その後、ランダムに選ばれた3つの診療と3つのインタビューにより信頼度を調査した。2人の盲検化された独立した評価者がデータのコードを高い信頼性をもって行い、84%の一致だった。この研究はマールブルグ大学医学部の倫理委員会で承認を得た。
Result:
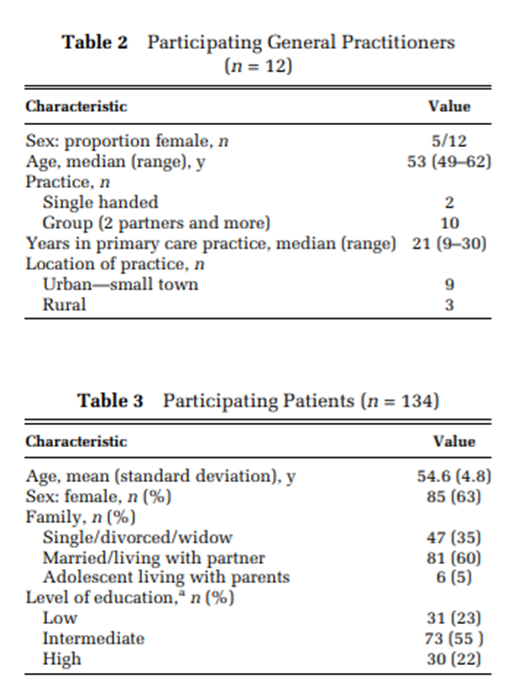
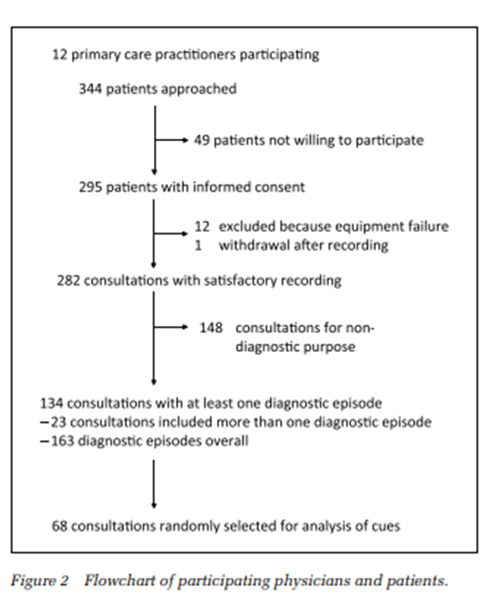
12人のGPのうち、5人が女性だった。平均年齢は53歳であり、プライマリ・ケアに従事した期間は2 1年だった(詳細はTable2)。除外基準にあてはまる診療を除くと、168回の診断エピソードを含む134例の診療が分析の対象となった(Figure2のフローチャート参照、患者の特性はTable3を参照)。
診療の平均時間は9分59秒(2分45秒から28分15秒)、インタビューは2分から18分の間で終えた(平均6分35秒)。
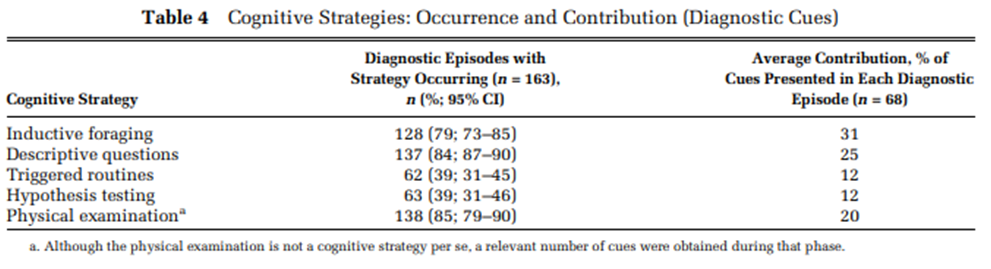
Inductive Foragingは122例の診療(91%)でみられた。残る12例のうち5例は技術的理由で診療の開始が録画されていなかった。この段階の所要時間の平均は34秒(6-176秒)であり、診断エピソードにかかる14.6%を占めていた。70例(57%)でGPが閉鎖的質問をなげかけることでInductive Foragingを終わらせていた。
私たちは限られた問題領域をGPが探索する診断プロセスの中間段階で特定した。Triggered Routinesは163の診断エピソードのうち、62回(38%)で観察された。Descriptive Questionsは137回(84%)観察された。身体診察は120例(89%)の診療で行われた。
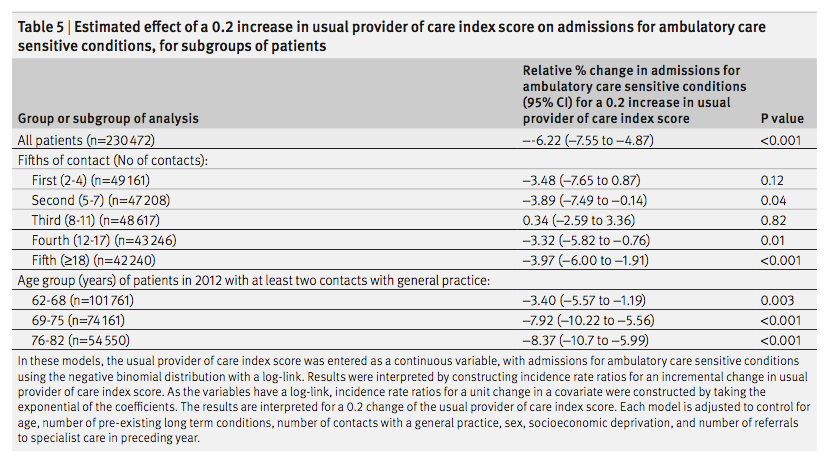
収集された情報から特定の疾患の確証と除外を行うことは仮説演繹法の優れた特徴である。しかしGPはこの方略を63回(39%)の診断エピソードでしか用いていなかった。量的に診断の手がかりについて分析したところ、inductive foragingは31%に寄与しており、仮説検証では12%しか手がかりを得られなかった。
Discussion:
134例の診療における研究で、GPはInductive Foraging、Triggered Routines、hypothesis testingを診断の評価の為に用いていた。今回のプライマリ・ケアの研究では、診断の手がかりを得るうえでオープンな方略は中心的な役割を果たすものの仮説検証の貢献は限られたものだった。
私たちの研究は、この分野のほとんどの出版された研究とは異なり実際の患者で調査を行った。プライマリケアの現場で発生する症状や病気に関する診療となっており、その結果、使用されているプロセスが患者の問題の全範囲にわたって反映されている。対象は経験豊富な実践者や教育に積極的に関与している側に意図的に偏っているため、経験豊富なGPの推論の詳細な説明を得ることができた。しかその認知プロセスは実際にプライマリケアに従事する医師と異なっているかもしれない。
研究された設定の自然性を保つための私たちの努力にもかかわらず、ビデオ録画とインタビューは、おそらくGPの行動や説明を妨げていました。私たちは、非公式のフィードバックと私たちの印象から、GPがより積極的で、より多くの仮説を立て、いつもよりも多くの情報を収集することがあることを学びました。その結果、我々の研究では仮説検定の頻度はおそらく過大評価されている。
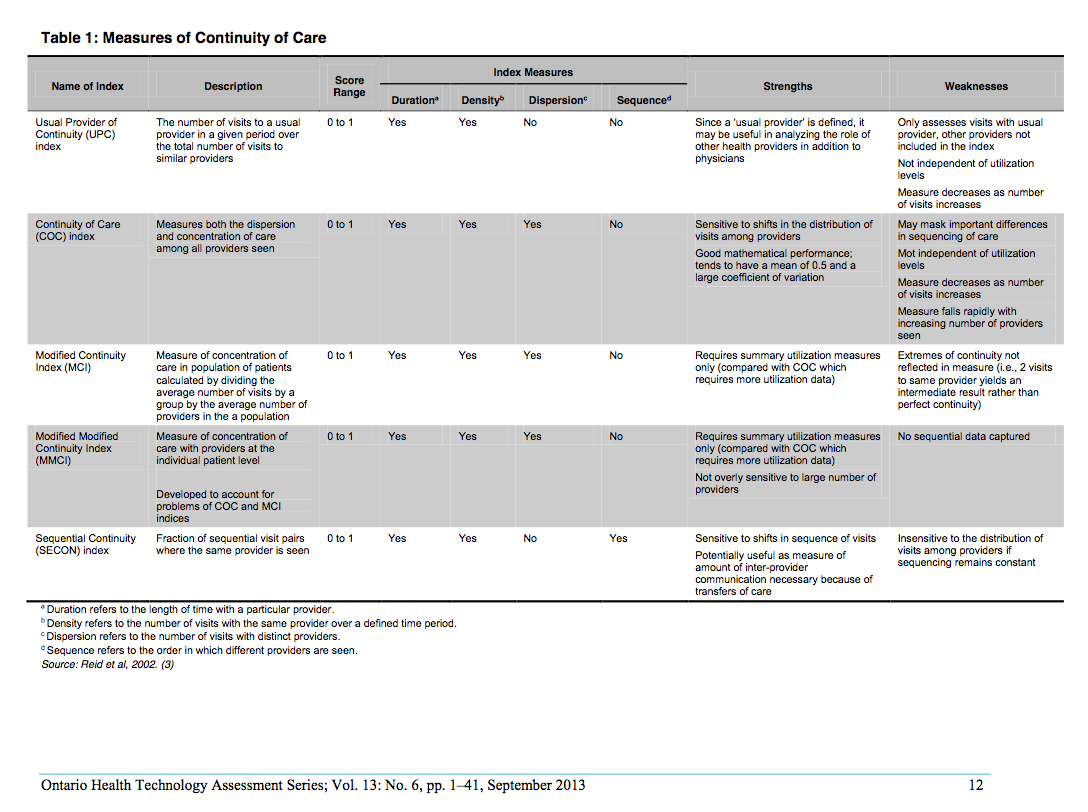
認知戦略の差異は必ずしも明確ではなかった。GPからの質問が、triggered routinesまたは仮説の評価として理解されるべきかどうかを判断することは時々困難だった。調査したコンセプトの明確な定義を繰り返し開発し、簡潔なフォーマットに落としこんだ(Table1参照)。これは、医学的に適格な観察者を訓練することと併せて、データ分析の高い信頼性をもたらした。我々は、身体検査によって得られた手がかりを別個に報告しているが、これは特定の認知戦略ではない。プライマリケアにおける身体診察は常に焦点が合っており、triggered routinesに似ている。
GPによって得られた手がかりの定量的調査は我々の研究の大きな強みであるが、関連性ではなくてその数だけの評価にとどまった。Triggered routinesまたはhypothesis testingによって得られた手がかりは、inductive foragingの間に提供されるものより診断にとってより重要だったと推測することができる。我々の研究は限られた数の側面に集中しなければならず、どのように医師が得られた知見のパターンを構築するか、感情、直観、または他の非分析的な戦略がプロセスにどのように影響するかは評価の対象にならなかった。
患者に最初のデータ収集プロセスを委ね、その後の段階でのみ介入することにより、GPは複数の診断可能性を有する設定に適応する。Inductive foragingは患者の苦痛感を緩和するだけでなく、診断問題の空間を定義するために不可欠である。患者中心の医療と診断的推論の世界は、それによって調和することができる。
【開催日】2018年9月5日(水)