― 文献名 ―
Marie-Claude Audetat, Suzanne Laurin, Gilbert Sanche, Caroline Beique, Nathalie Caire Fon, Jean-Guy Blais and Bernard Charlin: Clinical reasoning difficulties: A taxonomy for clinical teachers Medical Teacher 2013 35: e984-e989
― この文献を選んだ背景 ―
あざいでは平成26年1、2月に再研修を希望している医師の研修受け入れが決まった。しかし、私自身のここ1年あまりの教育活動は医学生実習と遠隔教育が主であり、医師研修受け入れについてはブランクがある。そのため、家庭医療コアの教育を行うチャンスは多くあったものの、臨床推論(※ここでは診断だけでなく臨床決断も含める)教育のチャンスは少なかった。
臨床決断において、困難な学習者がぶつかる問題、その診断とアプローチについて体系的に捉え直すことの重要性を感じていたところ、アクションリサーチの手法を用いて教育車向けの体系的なガイドを作成した研究を見つけた。最終成果物のガイドは非常に包括的で実践的であるため、是非共今回のジャーナルクラブで共有したい。
― 要約 ―
【背景】
臨床推論は医学実践での基盤である。現時点では、臨床推論における困難さ、その特定の方法、教育での改善方法についての確立したフレームワークは存在しない。
【目的】
①学習者の外来、ケースサマリー、カルテの評価の際に、最も頻度の高い臨床推論の困難さを特定すること
②医学教育者が、学習者診断とマネージメントをこの領域において行う際に助けとなるガイドを開発すること
【手法】
①概念的枠組み;以下の二つを採用した。
1.A parallel between the processes of clinical reasoning and educational reasoning.
臨床教育者が学習者を指導する際に、患者の臨床推論と学習者診断を同時並行で行っており、そのプロセスはい ずれも問題解決的思考(情報収集→仮説形成→診断→対応)という点で共通しているというモデル。
2.恊働構成プロセス
研究者が第三者的に観察するのではなく、対象である臨床教育者を随所で巻き込んで、研究をを進める枠組みで、具体的なリサーチデザインとして参加型アクションリサーチを採用。
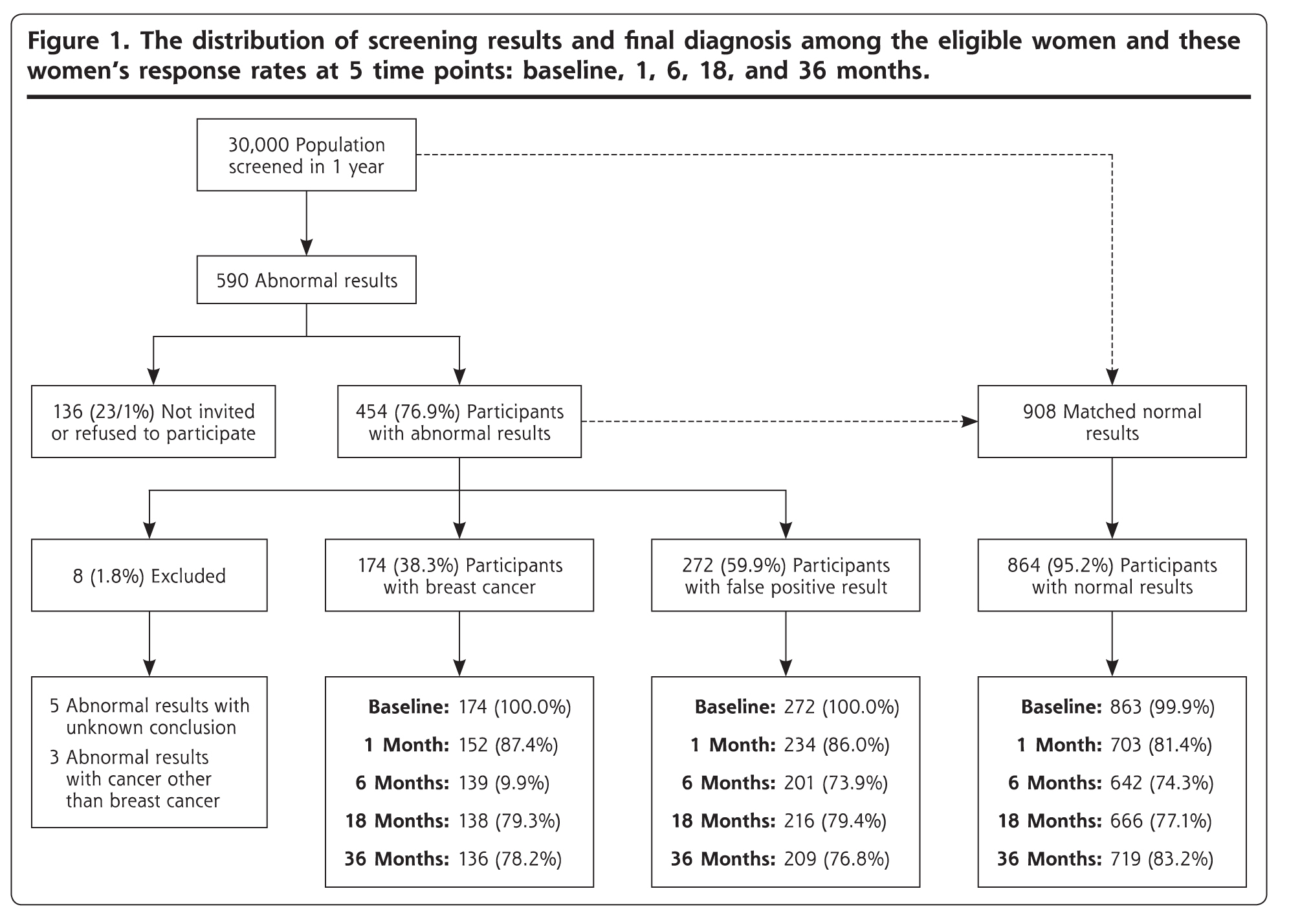
②セッティング;家庭医療レジデンシーを選択した。理由としては、診断上の不確実性と診断の誤りや遅れが多い科トップ3の一つだからである。
③参加者
モントリオール大学における家庭医療学・救急医学において医学教育に携わっている家庭医4人を選抜した。基準としては1.15年以上の臨床家・教育者としての経歴 2.臨床推論で困難なレジデントに関わる委員会に関わっている 3.FDの委員会、活動に関わっている 4.臨床推論における困難なレジデントの特定・改善プログラムに携わっている を考慮した。
④研究プロセス
参加型アクションリサーチに代表される方法で、計画–行動–観察–振り返りというサイクルを行った。具体的には、2009年4~8月の間に3時間のセッションをくりかえし行った。この3時間セッションの中ではテーマに対する振り返りと抽出を行った。セッション同士の間の期間で、参加者である臨床家がセッションで見いだした計画を実行し、観察を行った。その結果を踏まえて更に3時間のセッションで振り返り・抽出を行う・・・というプロセスを繰り返した。データが飽和するまで行い、8回のセッションが行われた。
ここでの結果をモントリオール大学のFDワークショップで共有し、17名の多分野の臨床教育者から妥当性の評価を受けた。
結果;先行研究を踏まえて、臨床推論のプロセスを以下の三つに分けて考えた。 1.仮説形成と情報収集の方向性 2.仮説の精錬と検証 3.診断あるいは問題の特徴付けとマネジメント計画
学習者が呈する臨床推論の困難さは1で1つ、2、3はそれぞれ2つずつの合計5つに集約された。それぞれについて、学習者が様々なスーパーバイズの場面において示す手がかり、特定するための問いの例、困難さの原因として考えうる仮説、困難さを改善するための教育戦略を特定した。それを集積したものを踏まえて、臨床教育者のためのガイドを作成した。
結論;このガイドは臨床教育者が、臨床教育の中で、あるいは特定の臨床推論の難しさを抱えた学習者に合わせた改善教育を施すにあたり、有益なツールとなるに違いない。
― 考察とディスカッション ―
質疑応答以外に以下のようなテーマでのディスカッションを行いたい。
・臨床推論につまづく学習者の評価を皆さんはこれまでどんな場面で行っていたか?
・皆さんが普段行っている学習者への問い、学習者診断、介入と比べてこのガイドはどうか?
・もし、サイトでこのガイドを取り入れるとすれば、どんな方法があるだろうか?
参照資料: CLINICAL REASONING DIFFICULTIES
http://informahealthcare.com/doi/suppl/10.3109/0142159X.2012.733041/suppl_file/0142159X.2012.733041.pdf
開催日:平成25年10月9日